“No! I don’t want to stop using.”
As therapists, we may or may not have encountered a resistant client or two. If you work with adolescents, resistance is part of the game. Some treatments are suited to deal with resistance, such as motivational interviewing (MI; Miller & Rollnick, 2012). There is even evidence that by just providing a contrast of people’s use of alcohol or drugs compared to a larger, more normative sample—this is called “normative feedback”—the stark difference can incentivize change. However, most of the studies that use some form of normative feedback were conducted with college-attending emerging adults. Unfortunately, we really don’t know if normative feedback is appropriate for or even works with adolescents. This article will review the effectiveness and mechanisms used in motivational interviewing how normative feedback has been wildly successful in college drinking literature. Further, an overview of a current study that asked the question “Is normative feedback appropriate for adolescents?” will be presented along with some potential clinical implications.
Adolescence is a period of autonomy, rule breaking, sensation seeking (Steinberg, 2007) and, more importantly, the time when substance use is initiated (Johnston, O’Malley, Bachman, & Schulenberg, 2013; Shih, Miles, Tucker, Zhou, & D’Amico, 2012). As a matter of fact, nearly 70 percent of adolescents report they have tried alcohol and nearly 50 percent have reported trying marijuana (Miech, Johnston, O’Malley, Bachman, & Schulenberg, 2015). Of more concern is adolescent binge drinking. Binge drinking can be defined in several ways, though the most common conceptualization is the consumption of five or more drinks for men or four or more for women in one sitting (Wechsler & Nelson, 2001). For example, adolescents may engage in binge drinking if they are “pregaming” for a party. In the United States, 23 percent of high school students report having been drunk in the past year, and 11 percent in the past month (Miech et al., 2015). Prior literature has identified several psychological (Harris et al., 2016; Jennings, Piquero, Rocque, & Farrington, 2015), behavioral (Craig, Morris, Piquero, & Farrington, 2015; Jennings et al., 2015; Miller et al., 2016), and neurological (Nguyen-Louie et al., 2015) deficits associated with adolescent binge drinking. For example, some studies have found that adolescent binge drinking can influence areas of the brain; in particular, the prefrontal cortex, which is associated with things like executive functioning, decision making, and impulse control. Some researchers have found that prefrontal cortex dysfunction is part of the neural basis for addiction (Krishnan-Sarin et al., 2007). And in some studies adolescents who report binge drinking have higher prefrontal cortex dysfunction than those who do not (De Bellis et al., 2005). All of these consequences have meaning when it comes to treating adolescents, but they also raise more questions: What type of treatment is best? Is there a way to mitigate these consequences of binge drinking?
These questions are difficult to answer. However, in the context of addiction treatment there are things that counselors can do when in session with their clients to aid in mitigating the potential consequences of substance use. That is, some treatments focus on eliciting client discussion surrounding change rather than drowning in the difficulties of why adolescents do not want to change. As researchers we have developed ways to pay close attention to what both clients and therapists say during sessions to help predict long-term outcomes. We will describe a study published in the Journal of Substance Abuse Treatment (Davis, Houck, Rowell, Benson, & Smith, 2016) that investigated the impact of MI and an added component of normative feedback among adolescents referred for a substance use treatment assessment.
Motivational Interviewing
MI is a nonconfrontational intervention that addresses ambivalence about behavior change through techniques such as empathetic communication and reflective skills. These skills are used to help elicit or reinforce client change talk and mitigate or minimize client sustain talk. So, what is change language? Change talk refers to “any self-expressed language that is an argument for change” and sustain talk is a “person’s own argument for not changing, for sustaining the status quo” (Miller & Rollnick, 2012, p. 159). For example:
- Client: “I got in trouble at school for smoking marijuana. It’s not a big deal, but my mom made me come here” (sustain talk).
- Therapist: “Well, I’m glad you’re here (affirmation), and it sounds like your mom means a lot to you (complex reflection), especially since you showed up today” (autonomy support).
- Client: “Yeah, I guess. I just don’t see the big deal about smoking weed” (sustain talk).
- Therapist: “So, you don’t see smoking weed as problematic, but it’s causing you some problems at school and your mom is a little worried” (double sided reflection: sustain talk and eliciting change talk).
- Client: “Yeah, I don’t like upsetting my mom” (change talk).
- Therapist: “You really care about her and don’t want to upset her. Maybe making a few changes would also keep you from getting in trouble at school?” (complex reflection).
- Client: “Yeah, you’re probably right. I’ve been in trouble a lot lately” (change talk).
In this example above we can see that the client is ambivalent about changing his or her behavior, however the counselor sticks with some key statements to elicit change talk from the client. This is important as several studies have found that when clients use more change talk in sessions they are more likely to change behaviors in the long run (Barnett, Moyers et al., 2014; D’Amico et al., 2015). Further, we can even use techniques that categorize client and therapist language. That is, we use a computer program to help a trained rater identify when clients are using change talk and when therapists are using MI-consistent behaviors, such as eliciting change talk. In these studies, researchers find that their clients are more likely to use change talk immediately after therapists use MI-consistent skills such as offering support, affirming, and emphasizing autonomy or personal choice and, conversely, more sustain talk after therapists use confrontational statements, giving advice or warn against their decisions (Gaume, Gmel, Faouzi, & Daeppen, 2008, 2009; Moyers & Martin, 2006; Moyers, Martin, Houck, Christopher, & Tonigan, 2009).
MI has been studied in over two hundred clinical trials (Miller & Rose, 2009) in studies involving samples of adults (Moyers et al., 2009), college populations (Borsari & Carey, 2000), young adults (Neighbors et al., 2010) and, more recently, adolescents (D’Amico et al., 2015) with a variety of problem behaviors such as medication compliance, gambling, and substance use.
Among studies that have investigated motivational interviewing with adolescents, Baer and colleagues (2008) found that when adolescents voiced reasons for change (compared to reasons for not wanting to change) they were less likely to use alcohol and other drugs one month later. However, the literature utilizing MI with adolescents and substance use is limited. To date, only five studies—six including the current study—have investigated the efficacy of client change talk with adolescents on subsequent treatment outcomes (Baer et al., 2008; Barnett, Moyers et al., 2014; Barnett, Spruijt-Metz et al., 2014; Engle, Macgowan, Wagner, & Amrhein, 2010; Osilla et al., 2015). Briefly, all the studies mentioned above found that MI, specifically change talk, had a significant influence on adolescent substance use. In particular, Baer and colleagues (2008) and Barnett’s studies (Barnett, Moyers et al., 2014; Barnett, Spruijt-Metz et al., 2014) found significant reductions in alcohol use up to a year later for adolescents who expressed more change talk during their sessions. Interestingly, D’Amico et al. (2015) looked at group level (i.e., adolescent group therapy) change and sustain talk and found that group change talk was associated with individual reductions in alcohol use, heavy drinking, and intentions to use alcohol.
Normative Feedback
Normative feedback is a way therapists can contrast an individual’s substance use to a larger, more normative, reference group. For example, some studies have utilized a national sample of treatment-seeking, age-appropriate, individuals for their normative comparison (CITE). An example of a normative feedback session would go as follows:
- Therapist: “I have some information that can compare your alcohol use with a larger, normative, sample of young adults your age. Would you like to hear it?”
- Client: “Sure.”
- Therapist: “You reported drinking five or more drinks in one occasion on fifteen out of the last thirty days. Among all kids your age in the US, only 5 percent reported drinking this much in the past month. What do you think about that?”
Here, you can see the therapist is contrasting the client’s current use with that of a larger, more normative sample. The idea behind normative feedback is many people, you and I included, tend to overestimate or misperceive how much and how frequently friends are using alcohol (Neighbors, Larimer, & Lewis, 2004). There is a vast body of research that suggests the larger the gap between your perception of peer use and our peers actual use is predictive of more problematic substance use (Borsari & Carey, 2001; Neighbors, Lee, Lewis, Fossos, & Larimer, 2007). This type of treatment additive has been widely popular among college drinking and drug use studies. For example, in a review of the literature on normative feedback interventions, Walters and Neighbors (2005) reported overall success among normative feedback interventions delivered either individually (e.g., Borsari & Carey, 2000), electronically (e.g., Neighbors et al., 2004) or through mailed information (e.g., Walters, 2000). Some studies even suggest that change talk is highest among college students assigned MI plus normative feedback (Vader, Walters, Prabhu, Houck, & Field, 2010). One question that has remained is “Is normative feedback appropriate for adolescents?”
Several studies have investigated motivational interviewing and normative feedback with adolescent populations (see Barnett, Sussman, Smith, Rohrbach, & Spruijt-Metz, 2012), but these studies have only investigated these effects when normative feedback is embedded in or a part of the larger treatment protocol. This is problematic, because we do not know if the normative feedback or the MI is the active ingredient helping adolescents reduce their substance use. As a matter of fact, some researchers believe that normative feedback may elicit a negative reaction among some adolescent groups—suggesting a “surprise” or “ambivalence” to the normative information provided. That is, if adolescents are provided contrasting information to what they believe (e.g., normative feedback is different than adolescents’ likely overestimated perception of their peers’ marijuana use), they may simply ignore this contrast and claim that their use is “normal” (Osilla et al., 2015). For example:
- Therapist: “I have some information that can compare your alcohol use with a larger, normative, sample of young adults your age. Would you like to hear it?”
- Client: “Sure.”
- Therapist: “You reported drinking five or more drinks in one occasion on fifteen out of the last thirty days. Among kids your age, only 5 percent reported drinking this much in the past month. What do you think about that?” (normative feedback).
- Client: “So what? My friends drink just as much as I do. These people are just losers or not like my friends” (sustain talk).
Others believe that adolescents may react negatively to normative feedback because of their higher psychological reactance compared to young and older adults (Barnett et al., 2012). This question about the appropriateness of normative feedback for adolescents has prompted some researchers to not use normative feedback in their interventions with adolescents (Winters, Fahnhorst, Botzet, Lee, & Lalone, 2012). As you may guess, if you had adolescents in front of you and they were to disagree with some normative feedback, it may result in counterarguments against the feedback. An adolescent’s reaction to this information may, in fact, result in more sustain talk which we know predicts worse outcomes (Baer et al., 2008). Unfortunately, no study to date had investigated the impact of the actual component of normative feedback among an adolescent population. With so much anecdotal concern, we sought to answer this question empirically.
Our Study
We conducted a randomized controlled trial that examined the impact of MI compared to MI plus normative feedback among adolescents who were attending a substance use assessment. To be eligible for the study, adolescents had to be between the ages of thirteen and eighteen years old and report using alcohol or other drugs on thirteen out of the past ninety days or score two or higher on the CRAFFT (Knight, Sherritt, Harris, Gates, & Chang, 2003). The CRAFFT is an instrument used to predict which youth may eventually be diagnosed with a substance use disorder.
We conducted baseline assessments with each of the eligible and consented youth, evaluating various psychological, social, and behavioral domains. After each of these initial assessments, youth were randomized into one of two groups: one that received MI only or one that received MI plus normative feedback. After youth were randomized, clinicians delivered the appropriate intervention based on the randomization results. Sessions lasted approximately thirty to forty-five minutes and were recorded so we could code both client and counselor language. All participants were assessed again three months later. At both baseline and the three-month follow-up, participants were asked about their substance use. Specifically, we were interested in four main outcomes:
- Days of alcohol use
- Days of binge drinking
- Days of marijuana use
- Treatment engagement (i.e., attending at least three treatment sessions)
How Do You Code Therapist and Client Language?
Our friends at the University of New Mexico Center on Alcoholism, Substance Abuse, and Addictions created a program called the CASAA Application for Coding Treatment Interactions (CACTI; Glynn, Hallgren, Houck, & Moyers, 2012). This program allows researchers to independently “code” each utterance—meaning every time someone speaks—in sequential order. That is, researchers are trained in a coding system known as the motivational interviewing skill code (MISC; Houck, Moyers, Miller, Glynn, & Hallgren, 2010). The MISC is a set of guidelines to aid in scoring each utterance on a variety of aspects. For example, therapists are coded on behaviors such as autonomy support, reflections, giving information, confrontation, and asking open questions, versus closed. For example,
- Therapist: “So, I see that your mom made an appointment for you. What brings you in today?” (gaining information).
- Client: “Yeah. I got suspended from school for smoking weed” (neutral).
- Therapist: “Ah, I see. So your mom is worried that you are getting into trouble at school so she thought it would be a good idea to talk with someone?” (simple reflection).
- Client: “Yeah, I guess so. I really don’t see the point, honestly. I’m not addicted or anything. I just like to relax” (sustain talk).
- Therapist: “I see. So, you aren’t worried about your marijuana use, but your mom is (simple reflection). However, it is causing some problems for you (complex reflection). How can we best spend our time today?” (autonomy support).
Further, clients are coded on similar behaviors such as change talk, sustain talk, and neutral language. The interesting thing about the CACTI software is it allows us to code in real time—thus we are able to code each utterance in the order in which it is spoken. Why is this important? This allows us to estimate the probability, or chance, that clients will use a specific type of language after a behavior by therapists. For example, our coding system creates probabilities that the statement labeled “A” will be followed by the statement labeled “B.”
- Therapist: “Tell me about your drinking.” (A)
- Client: “I don’t really drink that much,” (B) “but I have been smoking a lot.” (C)
What Did We Find?
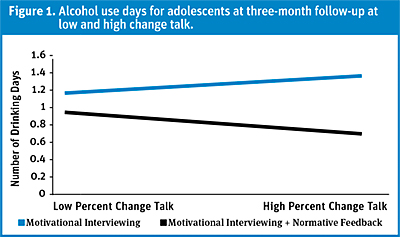
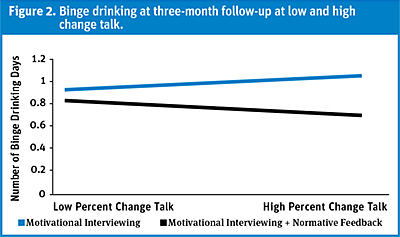
Once we had each session coded, we assessed the differences between youth assigned to MI versus those assigned to MI plus normative feedback from baseline to three-month follow-up. To do this, we looked at an interaction between the amount of change talk from each adolescent and which group they were assigned to. In Figure 1 we can see that adolescents assigned to the MI and normative feedback session had lower alcohol use than those assigned to just MI. Similar results were found for binge-drinking days (see Figure 2). However, if we take a closer look we see something that is much more interesting. You might notice a larger gap between the two lines at the right side labeled “high percent change talk” compared to the left side labeled “low percent change talk.” What this means is that adolescents assigned to MI plus normative feedback with high change talk during the session had significantly less alcohol use and binge-drinking days compared to all adolescents assigned to just MI and adolescents in the same group (i.e., MI plus normative feedback) with low change talk. Interestingly, we did not find any significant effects for cannabis use or treatment engagement.
Practical Implications
So, is normative feedback “bad” for adolescents? Our results suggest that the answer to this question may be more complicated than we initially thought. The answer involves a variety of components including within-session change language. That is, we found that adolescents assigned to MI plus normative feedback who had high change talk had a significantly lower number of alcohol- and binge-drinking days than those assigned to MI alone. If we think about these results in terms of practice, things start to make a little more sense. It may be that for adolescents with periodic or episodic binge-drinking episodes, the combination of having high amounts of change talk and normative feedback is enough to mitigate continued increases in binge drinking.
For the clinician, this has several implications. First, identifying heightened change language in a session may be a clue to utilize normative feedback, especially if your clients are showing increasing binge or alcohol use days. It may be that for these adolescents with high change talk, a heightened awareness of their non-normative behavior (e.g., a discrepancy between their current use and what they believe their friends use to look like) may be a “wake-up call” for them to consider cutting down. Reducing days of binge drinking, even by one event, is vitally important for adolescents given that their brains are still developing and the vast amount of research suggesting long-term dysfunction for adolescents who engage in binge drinking. For example, studies of adolescents with alcohol use disorder show smaller white and grey matter in the prefrontal cortex compared to adolescents without alcohol use disorder (De Bellis et al., 2005).
As a matter of fact, we have another study that is currently in the revision process that looked at adolescent binge drinking, impulse control, and victimization from age thirteen to age twenty-six. The sample was nearly 1,500 juvenile offenders followed for seven years. We found that during adolescence, increased binge drinking was associated with decreases in impulse control—remember, impulse control is a neurological function in the prefrontal cortex. Further, for those adolescents who experienced victimization, they were also more likely to experience deficits in impulse control. The interesting findings were, when adolescents transitioned into young adulthood—that is, ages eighteen to twenty-six—these patterns from binge drinking and victimization in adolescence carried over to young adulthood such that they experienced increased binge episodes and more victimization as they got older. There have even been studies that have investigated the influence of client change language on the brain. One study used magnetoencephalography to measure neural responses when participants listened to their own change talk and found activation in the right-hemisphere network indicating that therapists that are able to evoke change talk are able to activate neural change, which may be associated with behavioral change (Houck, Moyers, & Tesche, 2013). Needless to say, finding ways to mitigate binge episodes among adolescents is vitally important, and the use of normative feedback for those expressing high change talk might be one way to do just that.
Now, you might be wondering about the other end of the spectrum; what about youth who do not display high change talk during the session? These youth may be susceptible to maintaining or even increasing their alcohol use and binge-drinking days. This may be explained by a stark contradiction between the information presented versus their prior perceptions about how their peers use alcohol and drugs, or these youth may simply have lower motivation to change. In this case, clinicians who are more adept with MI skills may attempt to elicit change talk in the midst of sustain talk. In our study, we also looked at how likely it was for our participants to use change and sustain language following therapist behaviors. We found that when therapists used behaviors consistent with good MI, change talk among youth increased. This created a cycle of more change talk such that when adolescents expressed change talk it was more likely to be followed by change talk. Conversely, as adolescents began to express sustain talk, it was more likely to be followed by sustain talk. However, this pattern ultimately must originate with clients; youth will quickly notice when clinicians attempt to force them into a discussion of reasons to change, and respond with understandable resistance.
Considered together with the other published MI studies on this topic, our study suggests that therapists may play a major role in predicting long-term trajectories for adolescents. Although normative feedback can be a helpful tool, sometimes it may be counterproductive. During MI sessions with adolescents, if therapists notice that the clients are primarily emitting change talk with very little sustain talk, it may be useful to move forward with a discussion of normative feedback, which will most likely result in additional change talk. However, when young clients are clearly ambivalent, talking about what they like about alcohol or marijuana and why it would be hard to stop nearly as much as they talk about why they might want to change, it may be better to skip any planned normative feedback. Instead, counselors might circle back to spend more time engaging with clients and focusing on what they want to do, rather than pushing forward with what may be a harmful discussion of normative feedback. In youth like those in our study, who were relatively heavy-using adolescents, this approach may help avoid increased substance use like we saw among youth who had a lower percentage of change talk.
Finally, it is worth remembering that MI is about the partnership between counselors and clients, not persuasion or even manipulation by counselors. Although youth who drink more heavily are at great risk of problems that can continue well into adulthood, behavior change can’t be forced. Youth will notice when counselors, even empathic and well-meaning counselors strongly skilled in MI, consistently change the subject to change talk or focuses solely on change talk even when adolescents are talking about what are, to them, very real reasons for continued substance use. Our results suggest that pushing forward with an agenda for change when clients are not ready to move forward can lead to continued or increased substance use.
References
Baer, J. S., Beadnell, B., Garrett, S. B., Hartzler, B., Wells, E. A., & Peterson, P. L. (2008). Adolescent change language within a brief motivational intervention and substance use outcomes. Psychology of Addictive Behaviors, 22(4), 570–5.
Barnett, E., Moyers, T. B., Sussman, S., Smith, C., Rohrbach, L. A., Sun, P., & Spruijt-Metz, D. (2014). From counselor skill to decreased marijuana use: Does change talk matter? Journal of Substance Abuse Treatment, 46(4), 498–505.
Barnett, E., Spruijt-Metz, D., Moyers, T. B., Smith, C., Rohrbach, L. A., Sun, P., & Sussman, S. (2014). Bidirectional relationships between client and counselor speech: The importance of reframing. Psychology of Addictive Behaviors, 28(4), 1212–9.
Barnett, E., Sussman, S., Smith, C., Rohrbach, L. A., & Spruijt-Metz, D. (2012). Motivational interviewing for adolescent substance use: a review of the literature. Addictive Behaviors, 37(12), 1325–34.
Borsari, B., & Carey, K. B. (2000). Effects of a brief motivational intervention with college student drinkers. Journal of Consulting and Clinical Psychology, 68(4), 728–33.
Borsari, B., & Carey, K. B. (2001). Peer influences on college drinking: A review of the research. Journal of Substance Abuse, 13(4), 391–424.
Craig, J. M., Morris, R. G., Piquero, A. R., & Farrington, D. P. (2015). Heavy drinking ensnares adolescents into crime in early adulthood. Journal of Criminal Justice, 43(2), 142–51.
D’Amico, E. J., Houck, J. M., Hunter, S. B., Miles, J. N., Osilla, K. C., & Ewing, B. A. (2015). Group motivational interviewing for adolescents: Change talk and alcohol and marijuana outcomes. Journal of Consulting and Clinical Psychology, 83(1), 68–80.
Davis, J. P., Houck, J. M., Rowell, L. N., Benson, J. G., & Smith, D. C. (2016). Brief motivational interviewing and normative feedback for adolescents: Change language and alcohol use outcomes. Journal of Substance Abuse Treatment, 65, 66–73.
De Bellis, M. D., Narasimhan, A., Thatcher, D. L., Keshavan, M. S., Soloff, P., & Clark, D. B. (2005). Prefrontal cortex, thalamus, and cerebellar volumes in adolescents and young adults with adolescent-onset alcohol use disorders and comorbid mental disorders. Alcoholism: Clinical and Experimental Research, 29(9), 1590–600.
Engle, B., Macgowan, M. J., Wagner, E. F., & Amrhein, P. C. (2010). Markers of marijuana use outcomes within adolescent substance abuse group treatment. Research on Social Work Practice, 20(3), 271–82.
Gaume, J., Gmel, G., Faouzi, M., & Daeppen, J. B. (2008). Counsellor behaviours and patient language during brief motivational interventions: A sequential analysis of speech. Addiction, 103(11), 1793–800.
Gaume, J., Gmel, G., Faouzi, M., & Daeppen, J. B. (2009). Counselor skill influences outcomes of brief motivational interventions. Journal of Substance Abuse Treatment, 37(2), 151–9.
Glynn, L. H., Hallgren, K. A., Houck, J. M., & Moyers, T. B. (2012). CACTI: Free, open-source software for the sequential coding of behavioral interactions. PloS One, 7(7), e39740.
Harris, J. S., Stewart, D. G., Krzyzaniak, S. L., Charuhas, J. P., Moon, K. C., Holdren, A. L., . . . Joy, S. A. (2016). Binge drinking despite consequences: The role of psychological dysregulation. Journal of Child & Adolescent Substance Abuse, 1–8.
Houck, J. M., Moyers, T. B., Miller, W. R., Glynn, L. H., & Hallgren, K. (2010). Motivational interviewing skill code (MISC) version 2.5. Retrieved from http://casaa.unm.edu/download/misc25.pdf
Houck, J. M., Moyers, T. B., & Tesche, C. D. (2013). Through a glass darkly: Some insights on change talk via magnetoencephalography. Psychology of Addictive Behaviors, 27(2), 489–500.
Jennings, W. G., Piquero, A. R., Rocque, M., & Farrington, D. P. (2015). The effects of binge and problem drinking on problem behavior and adjustment over the life course: Findings from the Cambridge study in delinquent development. Journal of Criminal Justice, 43(6), 453–63.
Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2013). Monitoring the future national survey results on drug use, 1975–2011. Retrieved from http://www.monitoringthefuture.org/pubs/monographs/mtf-vol1_2011.pdf
Knight, J. R., Sherritt, L., Harris, S. K., Gates, E. C., & Chang, G. (2003). Validity of brief alcohol screening tests among adolescents: A comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcoholism: Clinical and Experimental Research, 27(1), 67–73.
Krishnan-Sarin, S., Reynolds, B., Duhig, A. M., Smith, A., Liss, T., McFetridge, A., … Potenza, M. N. (2007). Behavioral impulsivity predicts treatment outcome in a smoking cessation program for adolescent smokers. Drug and Alcohol Dependence, 88(1), 79–82.
Miech, R. A., Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2015). Monitoring the future national survey results on drug use, 1975–2014: Volume I, secondary school students. Retrieved from http://www.monitoringthefuture.org/pubs/monographs/mtf-vol1_2014.pdf
Miller, P. G., Butler, E., Richardson, B., Staiger, P. K., Youssef, G. J., Macdonald, J. A., … Olsson, C. A. (2016). Relationships between problematic alcohol consumption and delinquent behaviour from adolescence to young adulthood. Drug and Alcohol Review, 35(3), 317–25.
Miller, W. R., & Rollnick, S. (2012). Motivational interviewing: Helping people change (3rd ed.). New York, NY: Guilford Press.
Miller, W. R., & Rose, G. S. (2009). Toward a theory of motivational interviewing. American Psychologist, 64(6), 527–37.
Moyers, T. B., & Martin, T. (2006). Therapist influence on client language during motivational interviewing sessions. Journal of Substance Abuse Treatment, 30(3), 245–51.
Moyers, T. B., Martin, T., Houck, J. M., Christopher, P. J., & Tonigan, J. S. (2009). From in-session behaviors to drinking outcomes: A causal chain for motivational interviewing. Journal of Consulting and Clinical Psychology, 77(6), 1113–24.
Neighbors, C., Larimer, M. E., & Lewis, M. A. (2004). Targeting misperceptions of descriptive drinking norms: Efficacy of a computer-delivered personalized normative feedback intervention. Journal of Consulting and Clinical Psychology, 72(3), 434–47.
Neighbors, C., Lee, C. M., Lewis, M. A., Fossos, N., & Larimer, M. E. (2007). Are social norms the best predictor of outcomes among heavy-drinking college students? Journal of Studies on Alcohol and Drugs, 68(4), 556–65.
Neighbors, C., Lewis, M. A., Atkins, D. C., Jensen, M. M., Walter, T., Fossos, N., . . . Larimer, M. E. (2010). Efficacy of web-based personalized normative feedback: A two-year randomized controlled trial. Journal of Consulting and Clinical Psychology, 78(6), 898–911.
Nguyen-Louie, T. T., Castro, N., Matt, G. E., Squeglia, L. M., Brumback, T., & Tapert, S. F. (2015). Effects of emerging alcohol and marijuana use behaviors on adolescents’ neuropsychological functioning over four years. Journal of Studies on Alcohol and Drugs, 76(5), 738–48.
Osilla, K. C., Ortiz, J. A., Miles, J. N., Pedersen, E. R., Houck, J. M., & D’Amico, E. J. (2015). How group factors affect adolescent change talk and substance use outcomes: Implications for motivational interviewing training. Journal of Counseling Psychology, 62(1), 79–86.
Shih, R. A., Miles, J. N., Tucker, J. S., Zhou, A. J., & D’Amico, E. J. (2012). Racial/ethnic differences in the influence of cultural values, alcohol resistance self-efficacy, and alcohol expectancies on risk for alcohol initiation. Psychology of Addictive Behaviors, 26(3), 460–70.
Steinberg, L. (2007). Risk taking in adolescence: New perspectives from brain and behavioral science. Current Directions in Psychological Science, 16(2), 55–9.
Vader, A. M., Walters, S. T., Prabhu, G. C., Houck, J. M., & Field, C. A. (2010). The language of motivational interviewing and feedback: Counselor language, client language, and client drinking outcomes. Psychology of Addictive Behaviors, 24(2), 190–7.
Walters, S. T. (2000). In praise of feedback: An effective intervention for college students who are heavy drinkers. Journal of American College Health, 48(5), 235–8.
Walters, S. T., & Neighbors, C. (2005). Feedback interventions for college alcohol misuse: What, why, and for whom? Addictive Behaviors, 30(6), 1168–82.
Wechsler, H., & Nelson, T. F. (2001). Binge drinking and the American college students: What’s five drinks? Psychology of Addictive Behaviors, 15(4), 287–91.
Winters, K. C., Fahnhorst, T., Botzet, A., Lee, S., & Lalone, B. (2012). Brief intervention for drug-abusing adolescents in a school setting: Outcomes and mediating factors. Journal of Substance Abuse Treatment, 42(3), 279–88.
Editor’s Note: This article was adapted from an article by the same authors previously published in the Journal of Substance Abuse Treatment (JSAT). This article has been adapted as part of Counselor’s memorandum of agreement with JSAT. The following citation provides the original source of the article:
Davis, J. P., Houck, J. M., Rowell, L. N., Benson, J. G., & Smith, D. C. (2016). Brief motivational interviewing and normative feedback for adolescents: Change language and alcohol use outcomes. Journal of Substance Abuse Treatment, 65, 66–73.